This text course is an edited transcript of the webinar, Therapeutic Strategies for Counseling Complex Patients within a Pediatric Critical Care Setting, presented by Michael Hoffman, PhD.
Learning Outcomes
After this course, participants will be able to:
- List specific strategies for improving communication with patients and their families.
- Discuss the potential impact of multicultural factors on patient and provider experience.
- Describe how strategies can be adapted for use with patients with significant medical complexity.
Introduction
My goal for this presentation is to leave you with specific, concrete skills and strategies that you can use in your clinical work and in your patient interactions. In terms of a roadmap for this presentation, we'll cover the following: a brief introduction about me and my background; general skills that can be used with all patients; considering developmental care; the importance of considering diversity within healthcare settings; engaging patients in behavior change; and case examples. It's important to consider diversity and multicultural identity, as it will help you to better understand your patients and the populations that you serve. When we're dealing with complex families and patients, really what we're discussing is behavior change. My plan today is to drill it down and be specific, rather than just cover theory.
I am a Assistant Professor of Pediatrics at Thomas Jefferson University, as well as a licensed clinical psychologist. My specialization is in pediatric psychology. When I work with families and children, I almost always work exclusively within a hospital setting, and with kids who have some sort of history of chronic medical condition and their families. I did my graduate training at the University of Miami. My research focused primarily around kids with deafness and hard of hearing, a lot of whom were going through the possibility of getting a cochlear implant. I've done my residency and my fellowship at Nemours AI duPont Hospital for Children in Pennsylvania, where I'm now a faculty member. My main focus has been working with kids who are deaf and hard of hearing but I've also worked within the cardiac intensive care unit, and done a lot of work on our inpatient service with our intensive care units (ICUs). Currently, I provide integrated psych services to our families. I often tell my patients, "While we have the medical team who's working really hard on behalf of your medical needs, my job is to come in and support you as a family (or support the patient if they're a little bit older), and help you with everything else." We know that our patients are much more than just their medical diagnoses, and we know that no one wants to be in the hospital and dealing with all of its challenges, especially if they're in an ICU setting.
Research on Parental Functioning
I'd like to begin with what I call a "connect to purpose" or a reason as to why these factors are very important by highlighting data on parental functioning within cardiac and NICU settings. For children with congenital heart disease, we know that 80% of parents experience post-traumatic stress symptoms, 30 to 80% of them experience severe psychological distress, and 25 - 50% have some sort of anxiety or depression. If you think about your rounds or going from patient to patient, that means that the vast majority of families and patients that you serve in ICU, are going to have some of these challenges, which underly all of your interactions with them. About 23 to 28% of parents who have had children in the NICU experience anxiety disorders. Most commonly, they will show symptoms of post-traumatic stress disorder (PTSD) or what some might refer to as post traumatic stress syndrome. These symptoms include: hyper arousal, which is being very alert and aware of your environment, and flashbacks to the NICU. I had a mother tell me that the on-hold waiting music in the ICU was very traumatizing for her because when she called the ICU she was always waiting to receive information. For that mother, just calling the hospital to schedule an outpatient visit caused her to experience flashbacks to when her child was in the ICU. Another symptom is avoidance of the neonatal intensive care unit (NICU). 52% of parents experience post-traumatic stress symptoms two weeks after an admission. A lot of families are sort of in 'survival mode' while they're in the hospital, and then once they get out oftentimes the gravity of the situation settles in and they experience these post-traumatic stress symptoms. Roughly 1/3 of parents experience depressive symptoms.
While this might not be new information, it is important to be mindful of when we're working with patients and their families. We're not getting parents and children on their best days, and they often have a lot of stress, depressive symptoms, and post-traumatic stress happening.
General Skills that can be Used with All Patients
Here are some general strategies and skills we can use with all patients.
Being a Person
The first skill is what I call "Being a person". As medical providers, we have millions of things we are thinking about at any given time. We've got a full list of patients to get through, multiple evaluations to conduct, and many other things on our to-do lists. We may be stressed trying to do all the different things that we need to do, and we may be bouncing around the room from room just trying to get through our lists. It is important to pause, take a moment to talk to each family, and "be a human being". I can't tell you the number of times I've been in patient rooms and a provider walks in. They scan the patient's badge, maybe administer a certain medication, check vitals, or otherwise begin their clinical work on the patient without communicating or introducing themselves to the patient/family. They may not have said, "Hey, how are you guys doing, my name is _____, is there anything I can do for you?" Taking a moment to introduce yourself, making eye contact and talking to the family can make a difference. It takes all of five seconds to smile and introduce yourself, but it can make a difference to the family when it feels like they have people who are serving them and not just coming in to poke and prod their child. And, given that families may have dozens of providers day in and day out, I make a point to re-introduce myself each time I meet with a patient and family.
Make a discussion outside of medical topics. Ask the patients how things are going. If there is an upcoming holiday, ask the patient if they're celebrating or how they are handling that. If they have a picture of the dog in the room, or you notice other things, ask them about it. Then, remember it on your next visit and bring it up again. This makes patients and families feel like a human being is actually interacting with them, and they are more than just a medical condition to be poked and prodded. It will go a long way towards improving patient satisfaction. All of us know these things, but sometimes we're so focused on all we have to do from a medical standpoint, that we're not thinking about these other factors.
Normalizing
The other tool that I as a psychologist use more than any other one is what I call normalizing. Normalizing is one of the most powerful tools you can use with a patient and their family. When a parent or a patient is in an ICU setting, they often wonder if their problems are unique to them. They're stressed, they're anxious, and they have all of these worries running through their heads. By normalizing, we say things like, "Yes, what you're telling me is common. A lot of parents are really stressed and anxious before their children have a procedure, and I would expect you to be." Another example might be, "Given everything that your child has gone through having a trach, I understand this would be really traumatic." Simply normalizing, acknowledging and validating what a patient and their parent is experiencing, can make a difference. It can also facilitate more conversation and dialogue with a parent who may disclose more information and more discomfort about what they're going through.
How do we normalize? For me, I use statements that may start with:
- "A lot of children will say..."
- "Many others frequently tell me..."
- "Given your history, I would expect..."
- "This is very common among other parents of children with this condition...."
Examples include:
- "A lot of children will say they're really scared before they get a cardiac surgery or they have another CAT."
- "Many parents frequently tell me that it's really stressful coming in and out of the hospital, especially caring for all their other children."
- "Yes, given your history of a trach I would expect it to be really difficult to hear about having another procedure."
- "It's very common among other parents of children with CHD to feel kind of depressed and stressed out, feel like you're on a roller coaster with a blindfold on."
Normalizing is pretty simple and it's straightforward. It tells the patient or the parents (families, caregivers, etc.) that you are listening to them, you hear what they're saying, and that some of their experiences are not unique to them. I also have times where I will normalize for a family even if some of the things that they say are not necessarily within the scope of what I traditionally hear. What you're doing is getting buy-in from that family to feel like they can talk to you, share some of their experiences and then feel heard.
Reflective Language
Along the topic of listening, how do you show your patients that you are actually listening to them, and hearing what they're saying even if you are just dropping in for a quick check? The way that you can do that is through purposeful use of reflective language.
Reflective language is telling a patient that you hear what they're saying, and then giving it back to them. These are all stems of a sentence that you can use when we are trying to practice reflective language:
- "If I'm understanding you correctly..."
- "It sounds like..."
- "What I'm hearing is..."
- "I get the sense that..."
- "It feels as though..."
Examples may include:
- "If I'm understanding you correctly, you've been feeling extremely stressed recently because the doctors haven't been able to give you a clear sense of discharge."
- "It sounds like you're really worried about moving forward with that procedure,"
- "What I'm hearing is you're excited to go home"
- "What I'm hearing is that you're super nervous about managing the trach, before we get nursing assistants set up with you."
If you use reflective language with a patient, one of two things will happen. You are either going to accurately reflect what they say, in which they will be like, "Wow, he totally gets it - he was listening and understands what I said, and I like that guy." Or, you will learn that you are not entirely on point. That's okay too because these sentences are set up to give the patient the power to offer corrective feedback to you. When you start with "If I am understanding" or "It sounds like" or one of the other examples, it is clear that you are not being presumptive that you understand exactly what they mean. Rather, you are indicating what you think you hear or understand and you are offering the chance for them to give feedback. It shows that you are open to hearing them. The patient might say, "Well, actually I meant more like this", and provide clarification.
When we reflect back to someone, you want to use a downturn at the end of the sentence instead of an upturn. An upturn is what we naturally do when we ask a question. An upturn would be used with the question, "Do you want fries with that?", whereas a downturn would be used to reflect back: "I assume you want fries with that." When we reflect back to someone, we're not using a targeted question; we're just making a statement, and we end it with a downturn.
Being a Person, Normalizing, and Reflective Language will immediately get you a lot of buy-in from families so that you will be able to offer support and advice.
Avoid Being the Finger-Wagger
This is also a critical and important strategy - Avoid being a finger wagger. Often when we think about our most complex or challenging patients, there is a common thread of wanting them to engage in behavioral change. That is, as a provider we want something to be different than it currently is with the patient.
Traditionally, that behavioral change might be better adherence to a medical protocol, it might be changes in diet, or it might be better managing some sort of respiratory treatment. Whatever it is, we are trying to engage them in some sort of behavioral change. Oftentimes our desire as providers is to jump in and provide information. We provide them with information so they know why they should do what we tell them to do. We went to school, we studied hard, we continued our education, and we stay up to date on the literature. We have all of this expertise and all of this knowledge that we want to give to families. There tends to be this power dynamic when we walk in the room, which is, "I have all the knowledge, I am the expert, and you should listen and do what I tell you, and if you don't do it, shame on you." As providers, we may get frustrated when we feel like families are not hearing or listening to what we are telling them. We can all think of those patients where we believe if they had only just listened to what we told them, things would have been much easier for them, or they would have managed the disease much easier. We get frustrated. However, extensive research has shown that education in and of itself is not sufficient to produce behavior change.
I will highlight this with an example for you. We've all had the experience of going for our annual physical to our primary care doctor, and they recommend some type of behavioral change. Maybe they want us to quit smoking, cut back on drinking alcohol, cut back on fasts food, or lose a few pounds. They may say, "Mike, you might want to join a gym and lose a few pounds." What is your reaction to lecturing? Oftentimes, it is not motivating for you to make a change. You may think "Yeah, I knew they were going to say that - that knowledge is not new to me." It may reinforce what you already know, but it does not necessarily motivate you to change.
In many cases, the people we are working with know the information we are going to share before we tell them. They may know that they're not doing a great job adhering to their medical protocol, or they may know they'll be advised that something needs to change. Think back to your own experiences as a patient in this situation. Providing education in and of itself does not inspire or motivate behavior change, particularly when we're dealing with more challenging or complex situations. Being the finger-wagger and telling someone, "You need to do this, and you need you to do that because I am the expert," just doesn't work.
Think of those times where you provided information and education, and you felt like a family should be listening, but they were not. What are the reactions that you've experienced when you're dealing with a challenging family, and you're providing education? The patient or the family may become defensive, they may become closed off, they may try to justify or explain their current views and behaviors, and they may feel misunderstood. When you get into the position of telling them what to do, then naturally, that puts the patient on the defensive. They may tell you why they are doing things the way they are doing them, and why they haven't been better about adhering to protocols or recommendations. When we get in this position of feeling that we are running opposite to our patients and experiencing head butting, we may leave feeling frustrated, and they are left feeling frustrated and annoyed. Be mindful of the fact that simply providing education in and of itself does not inspire behavior change. The strategies we've discussed up until this point including leaning in, being a person, and engaging in reflective listening, will buy you a lot of clout and a lot of buy-in from the families. Let's now discuss how to flip some of these situations around.
Roll with Resistance
When we are talking about those moments that you go into a room and experience a lot of pushback from the families, in psychology we call that resistance. If you find yourself experiencing resistance, or on the opposite side of a discussion with a patient, ask yourself, "How can I roll with this resistance? How can I get myself back to a place where I'm aligning with the family, rather than going against them?"
The strategies for rolling with resistance include: Call it out, gather more information, and find a middle ground.
As soon as you find yourself in a position where you are the lecturer, and you are talking at them, is the moment that they are no longer engaged in wanting to do what you are telling them to do. If you find yourself having that tension and your gut feeling is that things aren't going well, pause, stop, and call it out. Calling it out can be as simple as saying, "I know I'm kind of talking at you a little bit about all of these things, and these next steps in medical care, but I can see maybe you're a little bit frustrated or annoyed. I was just hoping can you tell me what's going through your head right now?"
Then, gather more information. You can ask these types of questions: "I know this is probably really overwhelming and you're getting so many things thrown at you. Can you tell me where you are, and how we might be able to help?"; "What do you think is the biggest challenge for all of these things that I'm discussing?"; "Do you feel like this is feasible?"; "Are there other factors at home that might be impacting you guys to kind of carry this plan forward when you get discharged from the hospital, or even in an outpatient setting?"
As providers, we sometimes have this idea of a gold standard. It's all or nothing, either the patient is hitting that gold standard and they're doing what they're supposed to do or they're not. The truth is, there's a whole middle ground in there. If we take the time to listen to them and hear what they are saying, we can often find some sort of compromise. In some situations, it may just be a specific protocol that has to be followed. Pausing, calling out the resistance, gathering more information, and working with the patient to find a middle ground, can be very helpful. Is there a compromise to be had?
You want patients, parents and caregivers to feel that you are empowering them, and that they are an expert in their child or in themselves. You want them to feel that they also have valuable information and feedback to offer. It is not that I am up here as the expert, and I am telling you what to do and you need to listen to me. You as the family or you as the individual have lived experiences, and I know the research and the literature, so let's figure out something together that works for you. We want to make patients and families feel that we are on the same side as them, and not rowing against them. We are working together both as experts in certain areas.
The most important takeaway from today's course is this: Don't be the finger-wagger. If you find yourself falling into that category of being the finger-wagger, take a pause. Put your finger down, call it out, gather information, and then figure out how to move forward.
How to Provide Information
Despite everything I just said before, we obviously need to provide information. We obviously have data that is valuable to share with parents and patients and caregivers. How are some effective ways we can do that?
Ask permission. One of the easiest things you can do to get buy-in is to ask permission. Asking permission is as simple as saying, "Is it okay if I tell you about...?". Once you ask permission, one of two things will happen. You may make the patient or the family feel like they are somewhat in control of their own visit again, in which case they will say,"Yes, you can give me more information, I would like to hear it." That creates a standard and expectation in their head, which is, "Well, I just told Dr. Hoffman that he can give me more information about the next steps in my trach treatment, so now I have to listen to what he will say." So simply getting someone to give you permission to tell them more about something, mean that they're more likely to listen and receive that information.
If they say no, which is very rare, then they're probably not ready to receive that information. They are not ready to move forward. If they say "no", it may save you some time from going into that finger-wagger role. It tells you to pause and stop, and gather more information.
We may give information to people in outpatient settings, but how we deliver information is also very important in critical care settings. When patients and parents are in critical care settings, they often feel that everything is being dictated to them. You will hear families say they feel they have no power in these situations. It feels chronically overwhelming. When we can give back a sense of control, even in a small way, it can bring a sense of stability for families.
Many parents will say they feel like they're on a roller coaster. I've taken that one step further to say, yes you're on a roller coaster except we don't know when the roller coaster will end, how long the ride is, and you're riding with a blindfold, so you have no idea if you are to go up or down. You don't know if it will be a good day, a bad day, if you will get thrown in a loop or if things will be calm. Finding a way to give some control back to parents can be very helpful.
Sharing information across providers. It is important to consider how we share information across providers. As a psychologist, I do have to be clear to families that not everything they say to me is confidential, as I do have to put notes into the medical record. As a respiratory therapist, when families share information with you, be mindful to ask if you can disclose that information to the rest of the team. You can ask, "Is it okay if I let the rest of the team know? Do you have any feedback I can give to the rest of the team?", or "Is this all right if I put the note about this in the chart?" Sometimes giving them a little control and talking to them about sharing information can be helpful when working with families.
I hope the information I have shared until now is a clear reminder, that we're not just treating the medical diagnosis. We want to make patients, caregivers, and families feel that we are there for them. We want to try to give them some control, make them feel like they have some say in what is going on, and communicating with them as people. We are not just focusing on a specific respiratory treatment, or cardiac issue, or intensive care setting.
Multicultural Identity
Multicultural identity should be considered with all patient interactions and family interactions. Culture and identity are integrated into everything we do. It is no longer okay to not pay attention to culture and identity. In the U.S. and in other countries, there are significant health disparities that exist, primarily for people who are black, indigenous, and others who may have minority status. We should always be thinking about ways in which inequities may exist in our hospitals or day-to-day work settings. It's not a question of if health disparities exist, but how, and in what ways do they exist? And, what are we doing to be mindful of them, and to address them to reduce inequities as much as possible?
Our Role
I believe our role is to serve as an advocate on behalf of families within the medical teams. Again, we are seeking to treat the patient and their families and not their illnesses.
How do we serve as an advocate? One example is by the language that we use. We want to model person-first language - we would refer to "a person with diabetes" and not to "a diabetic", for example. The way we acknowledge and identify barriers to care is also important. It is our role to call out differential handling of patients. I'm sure any one of you could pause and think about times where maybe one family received a certain higher level of care, or better treatment than others. Be mindful of moments when differential handling to patients is occurring, and do not be afraid to call that out. Have courageous conversations. Recognize and identify issues of medical mistrust. For many families, particularly families of color, there's a long insidious history in this country around issues of medical mistrust and medical abuse. If you've read about Henrietta Lacks or know about the experiments at Tuskegee Institute, these are just a few examples. And, think about statements of frustration. If patients or families are making statements of frustration, get feedback and ask, "How can we help?" And, think about statements of frustration from providers towards families. Many times, I've walked out of a patient's room and encountered another provider. With the family and patient within earshot, the provider has expressed frustrations and difficulties about the family and asked me to help them. It's important to move to a private place away from the patient and family to have these types of conversations.
Why This Matters
We should always strive to consider the intersectionality between multicultural identity, and the experience of an illness, disability, or an acute hospitalization. Studies show that white, well-resourced families experience hospitalizations, medical treatment and illness very differently than individuals and families of color, and than those with less resources (Williams & Cooper, 2019; Baumann & Cabassa, 2020; Adler, Glymour, & Fielding, 2016). Many times when we are experiencing challenging situations with complex patients, some of these multicultural factors, maybe playing a role.
The Role of Multicultural Identity
The role of multicultural identity refers to all of the factors you see in Figure 1.
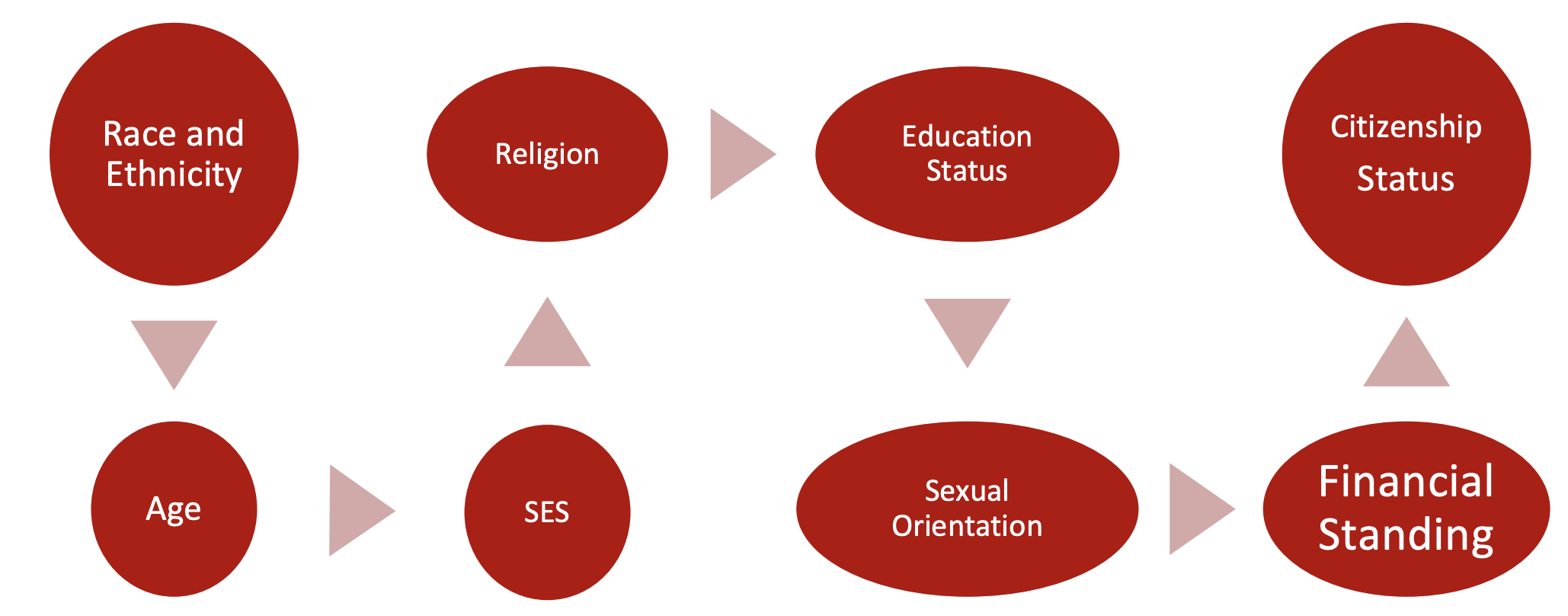
Figure 1. Multicultural identity - factors.
As providers, we bring our own background, lived experiences, and perspectives into the room. The patient also brings their own experiences, their own background and their own perspectives in the room. If you sense resistance, consider how some of these factors might be at play. These factors can be crucial to helping get to a better level of understanding and support for the family, versus continuing to experience frustration and irritation with them.
Here is an example. Let's say I am working with a family who has a medically complex child with sickle cell anemia, and they are a black family. I walk into the room and say, "I know how challenging it must be for you." That family might feel that I, as a white male, have never been in their position, don't have sickle cell, probably don't have family members who are dealing with sickle cell, and have no idea how challenging it is for them. Stopping to acknowledge that fact such as by saying, "I don't know how hard it must be for you, I've never dealt with sickle cell myself personally or within my family, and so I'm not going pretend that I know exactly what it's like. I'm wondering if you could share some of your experiences with me?" That is a perspective of cultural humility, rather than just throwing out the phrase "It must be hard."
Thinking about some of these factors and these challenges when they come up are really important. Even if you don't call them out, they're still there. It's not a matter of whether they exist - it's a matter of whether you're going to acknowledge them or not. Most families appreciate when you call out challenges that occur. If you have a patient whose citizenship status isn't clear or who may be undocumented, it obviously can impact a lot of things like access to additional medical care and follow-up outside the hospital. You can say, "There are ways we can help with this," or, "This must be really stressful in that regard."
It's also important to acknowledge and talk about intersectionality. If you're not familiar with this concept, intersectionality is a meeting point of various cultural identities, such as race, gender, medical diagnosis, and any other factors. Think about yourself, and the intersectionality of your race and ethnicity with your gender, the intersectionality of your education and the part of the country that you live in, or the intersectionality of the cultural values of the hospital system that you work in with your own religious beliefs. Intersectionality is constantly happening.
Another point to keep in mind is that experiencing disability or experiencing a challenge, does not mean you don't have privilege - both can exist. I happen to be deaf and hard of hearing, and I have a cochlear implant. I have a lot of privilege in the way that I experience my own hearing loss. I never had to worry about access to care or getting to and from appointments, and I never had to worry about being able to afford a hearing aid repair or new hearing technology. I knew my parents could generally make it work, though it might be stressful for them. In my own experience as a deaf individual, I have a lot of privilege because I also still benefit from being a white, relatively well-resourced male.
I know I'm going a little bit into the weeds here but in thinking about our patients, and our families as people, then these are important factors to acknowledge and discuss. When we're dealing with complex families and challenges, these are things that come into the room.
Microaggressions
Another thing that I've heard and seen on the medical team is what I would call microaggressions. Microaggressions are indirect, subtle, or unintentional discrimination against members of a group. For instance, someone said to me, "Wow, you speak really well for a person with hearing loss." I've heard people say things like, "I can't believe that you have a cardiac diagnosis, I never would have guessed." Or, "It never seems like you struggle that much with these things." Sometimes there are these small little digs that happen and people don't even realize they're doing it. I've heard a microaggression described as "a raindrop that doesn't know it is part of a typhoon".
As providers, we may not realize the broader context around these comments we make about patients in front of them or towards them. They can have a negative impact despite our positive intentions. Microaggressions can contribute to the experience of chronic race-based stress in Black and Indigenous People of Color. Be mindful of them because they exist and they're happening - it's not a matter of if, it is how and when.
Implicit/Unconscious Bias
Implicit or unconscious bias is another consideration when working with families. If you are skeptical around this topic, I strongly recommend taking the implicit bias tests that are available as part of Harvard's Project Implicit (here is the link). There is a lot of research that links implicit or unconscious biases to explicit behaviors that people engage in. For instance, a study from the Harvard group looked at implicit bias in physicians in their interactions with caregivers during appointments. Those who showed stronger preference for white families versus black families were much more likely to ask less questions gather less information, and spend less time with patients of color, than they did with white families. There is a lot of data about implicit biases and it is beyond the scope of this presentation to get into further details. However, I encourage you to look into it on your own, reflect on your trigger points, and consider how it may play into your work with families and patients.
Communicating with Children
Many medical providers, and also caregivers, ask about how to communicate and share information with children in complex medical situations. How do we talk to them about what's going on? I think the gold standard is, if a child is old enough to ask a question about what is going on with their own medical care or their medical needs, they are old enough to receive the answer. If that question does come up, be open and be honest with the child. Match their developmental level, and that might require being broad or simplified. For example, if a child is asking questions about something like a trach, don't be afraid to answer their questions and talk to them about it. However, the child doesn't need to know all the specific nuances and details of what is involved. I've been guilty of this myself, sometimes we want to back off from questions from children. We may think, "I do not want to talk to this kid about that." It may be my own discomfort that is preventing me from having that conversation. But keep that standard in mind - if a child is old enough to ask a question, they're old enough to receive the answer (matched to their developmental level).
Developmental Care Approach
There is a lot of research coming out about developmental care approaches in the intensive care unit. This refers to a wide range of interventions designed to individualize care and minimize stress for infants to maximize their neurologic development (Sood et al., 2016). That includes things such as controlling the external environment (vestibular, auditory, visual, tactile), regulatory infant support, or nonpharmacologic comfort measures. More importantly, this refers to family integrated care that cultivates parents' capacity to observe, understand, and respond to their infants' states and behavioral cues to promote more optimal infant regulatory functioning.
Regarding giving parents control, think about the example of an infant's first feeding. If providers go in and start feeding a child right away, the parent never gets that opportunity to be involved in the first feed. Maybe they were sleeping or not present. For mothers, breastfeeding may be a deeply personal experience. Many mothers are upset and sad about the fact they might've missed their first feed. The same for being able to change diapers or otherwise be involved in their child's care. We need to understand that parents can observe and they can respond to their child's cues, and they can help out with their child's state. That may be as simple as holding the child's hand. Giving parents some sort of control over what is happening during an admission can lead to optimal infant regulatory functioning.
I encourage you to always ask yourself, "Are there ways in which I can involve this parent into the patient's care?" At our hospital's CIC, we had developmental care rounds which brought together all of the providers involved in a child's care including OT, PT, Speech, feeding, psychology, social work, child life, nurses, and physicians. The goal was to discuss how families' experiences can be maximized, and to help families know how they can care for their child in a given time. We also discussed challenges that may arise towards discharge, and reviewed any other issues that would come up. These rounds took us away from the medical focus, and got us talking about the whole patient. Obviously, the medical focus is important, but thinking about the families and the patients is equally valuable.
Engaging Patients in Behavior Change
The last area we'll cover in today's course is engaging patients in behavior change.
Prochaska and DiClemente's Stages of Change Model
This model has been out for almost 40 years now, but it is still very much relevant. The idea with this model was that there are six different stages of change:
- Pre-Contemplation: no intention on changing behavior
- Contemplation: Aware problem exists but with no commitment to action
- Preparation: Intent on taking action to address the problem
- Action: Active modifications of behavior
- Maintenance: Sustained change, new behavior replaces old
- Relapse: Fall back to old patterns of behavior
It's very helpful to think about where a patient might be in their stages of change, in order to facilitate the way that we talk and engage with them.
In Pre-contemplation, the patient has absolutely no intention on changing their behavior. They have no intention to better manage their respiratory needs or take their medication. Jumping in to tell them all the things they need to change may not work well.
Once we move past Pre-contemplation to Contemplation, a patient may be aware of a problem and know it exists. They may have thought about committing to action but they don't have a specific plan or process in place.
After that, a patient moves into the Preparation phase, which means that they're actually intent on taking action to address a problem and make a behavior change. They haven't actually taken steps to do that behavior change but they're coming up with a more crystallized clear plan.
Action is when they start to engage in some behavior change. They're taking steps to modify the issue.
Maintenance is, "I've made this change, I'm engaging this change, and I'm maintaining it for a while."
Relapse can happen where you fall back, relapse, and stop doing that change.
When we are dealing with families, particularly complex ones, and we want them to change their behaviors or get them to do something different, it can be very helpful to consider which of these stages they are in. If I am trying to get a patient to Action, maybe that patient is actually still in Pre-contemplation and they're not even acknowledging that this issue that you're trying to address is a problem. Trying to jump them to Action and skip three or four steps is not going to work well. Acknowledge where they are and maybe just have a super brief conversation at that time, to move them from Pre-contemplation to Contemplation. Then, next time you keep going based on which stage they are in.
Eliciting Change Talk
Let's discuss some of the ways that we might engage a patient in change talk. Behavior change is not just education; it is actually motivation and willingness to engage in change.
Eliciting change talk is one way to engage someone to change their behaviors. The "Motivational interviewing" by William R. Miller and Stephen Rollnick is a great resource. I recommend you read it - you don't need to be a psychologist or a therapist to benefit from the information.
In the book is an idea to ask a patient to rate themselves where they are, on a scale of one to 10. We think that most patients have some sort of ambivalence about behavior change. They may not be 100% on board with change or against it, and maybe they can articulate and explain a couple of reasons why they might go either way.
For example, say a patient needs to undergo a certain procedure, and they're resistant towards it. I can use scaling by saying, "If 1 = I will never have that procedure, absolutely not, and a 10 = Yes, I want that procedure right now, where are you on that scale?" The patient's answer will give you a sense of where that patient is with their decision. They may tell you that they're at 3, and say something like, "You know I really don't want to move forward with this new surgery, I'm at 3." I can then pause, and ask some questions. I can ask them why they are at 3 and not at 1. If I say something like that, then the patient or caregiver can explain and detail the reasons why they're not lower. In other words, they have to argue for the change (from 1 to 3). True behavior change comes from increasing motivation and getting a patient themselves, talking about the reason of why they want to engage in a change. If they say, "Well I'm a 3 and not a 1 because I know this would probably be really helpful for me, and make my breathing easier most likely." Now you're getting that patient discussing reasons for change.
You can also get them to discuss reasons for change by asking them, "What makes you think you need to change?" With teens, one of my favorite questions to ask is "Why do you think your caregiver wants you to do this? What do you think they would say if we asked them?" Again, it gets the person talking about the reasons for change. Then you can ask if they agree with the caregiver.
You can also ask what the patient thinks will happen if they don't change. Ask them what would happen if they don't go through with the procedure. They may list things like they could be re-admitted, or might not be discharged. Get the patient to talk about the reasons that they do not want to maintain their current challenges.
Another question you can ask to elicit change behavior is, "Do you think others are concerned about your behaviors, and why?" I use the example of caregivers, but it could really be anyone.
Finally, you could have this conversation from the other direction. If the patient says they are a 3, ask what it would take to move them to a 7, for example. Ask what barriers there are to move them to a 7 and what you can do to help them. This gets them talking about what else needs to happen or what else needs to change to get their motivation to increase over time.
This has been a quick recap of motivational interviewing and change talk, but it's definitely worthwhile to think about and read about. The whole idea is to get on the side of your patient, roll with the resistance, and get them talking more about the reasons that they want to engage in a change, rather than not.
Case Example
Let's look at an example of a 15-year-old male, Charlie, who is a cardiac patient. He needs another critically important medical procedure, a VAD. He is being extremely resistant to the idea of moving forward with the VAD even though it is very important from a medical standpoint.
One of the ways that I can have a conversation with this patient and his family, and to try and understand where they're coming from, is to get them engaged in change talk. Here is a sample dialogue:
Me: "All right, help me understand when you're talking about getting a VAD, like on a scale of one to 10, where would you say you are? 1 = No way, never in a million years, absolutely not, and 10 = Yes, let's do it for sure. Where would you say you are?"
Charlie: "I don't know, I'm like a 4 - I really don't want to do it, I just don't want to have this procedure."
Me: "All right, well, I really appreciate you sharing that with me and telling me that you're four. So it sounds like a four means you're a little bit against it. You're probably more against it than you are for it at this time, does that sound about right?
Charlie: "Yeah,"
Me: "Okay, well, thanks again for sharing that with me. Can you tell me why you're a four and not like a two?"
Charlie: "Well, I know that things are getting worse, like my heart functioning is not doing well, and the doctors are saying I should get this. I don't know, that seems to be the main case. I know if I do get it, it could make things better for me."
Me: "Okay, it definitely seems like they think this would benefit you and possibly help you moving forward. So, I guess, can you explain to me like a little bit more about why you're a four, and not like a seven or eight, because it sounds like you know that this is really important?"
(As an aside here, I'm looking for some of the barriers and the challenges).
Charlie: "Well, I mean I really don't want to have this backpack thing that I have to carry around all the time and charge the batteries. I'm not even really sure I have an understanding of exactly how it works. It just sounds pretty bad. I won't be able to do a lot of the activities I like to do like play football and stuff."
Me: "Yeah, so it sounds like this recent change of not being able to engage in physical activity is really hard, and it feels like getting the VAD is going to only make that even more true, that you can't really do a lot of the things you wanted to do before."
Charlie: "Yeah"
Me: "And it also sounds like, you're still not entirely sure how the VAD works, but having to wear it and wear the backpack and carry the batteries sounds pretty overwhelming for you."
Charlie: "Yeah."
Me: "Well, I guess I'm wondering what can we do to get you from that four to a seven or an eight? Is there anything that you think would be helpful?"
Charlie: "Well, I feel like I just need time to think about it. Maybe someone can explain it better to me and talk to me about why I need this in the first place."
Me: "Sure. Is it okay if I give you a little bit more information about why that might be helpful, and why the doctors are talking about this?"
Charlie: "Yeah, that would be really cool."
Me: "And then we can also maybe talk to them about some of your concerns. Is it okay if I share that with the team?"
Charlie: "Yeah."
In this case example, instead of jumping in and being that finger-wagger, I try to talk to the patient and understand them. We talk about why that a certain procedure might be helpful and get a sense of what the barriers are, what some of the challenges are, and what some of their reasons are for moving forward. What I didn't do in this case example was start with, "Why do you think you need to get the VAD? Why does your mom feel like it's important?" In this case, it became clear that a barrier was that he didn't have a lot of information around the procedure. I asked his permission to talk more about these things, and then give more education around that.
Regarding scaling, notice I started asking about 1 to 10 in an exaggerated way, with 1 being "No way, never in a million years". I want to encourage them as much as possible to go towards the middle of the scale. If I say a 1 means "you don't want to do it" then a lot of kids will say they are a 1 and it is harder to move up the scale. By saying, "Absolutely not, never in a million years", then I'm trying to make it really extreme to go towards a 1. And the same with the way I describe a 10.
When I teach this people will ask me, "What if the patient says they are a 1?" It is pretty rare that someone will say they are a 1. If they do say they are a 1 about engaging in some sort of behavior change, then that is a lot of information they are giving you. As providers, that tells us they are just not there yet. Rather than try and push them to get them to understand why they should do this, I can pause and think back to the stages of change model. They are in the Pre-contemplation stage. I can figure out how to work around that, rather than jumping all the way to the Action phase.
The overall takeaway is that when we are dealing with families, we want to avoid being a finger-wagger and lecturing, because it does not work to motivate change. Our goal is to align with the patient, family and caregivers, to be supportive, and to help them with these challenges so that they can move forward.
References
References are included in the handout.
Questions and Answers
Have we begun to understand why some patients or families develop PTSD and others do not?
That's a good question, and the short answer is not really. It is multifactorial, meaning that the way that someone responds to any given situation has many different factors that go into it. For example, a previous history of PTSD is a factor. If a parent lost a child before, if they've had their own trauma, or their own abuses that they've gone through, they will be more at risk. Think about the different types of codes that a child might experience in the course of a hospital admission. Whether the parent was there or not may impact the way that they understand the information of what's going on with their child or what we would call health literacy. We've all had patients and caregivers who can understand what is happening at a very high level, and those who don't have quite as much knowledge and understanding of things. These are examples of factors that might go into how someone responds to a given situation. Other factors include extended support, spousal support, and family support. We don't have an answer just yet of exactly why some develop PTSD and others do not. We do understand some of the protective factors and risk factors. I think the best thing we can do is be aware of such factors. Know that PTSD rates are high with our patients and families, and recognize that the behaviors of our patients and families may be due to stress, anxiety and depression.
What is the best way to educate the interdisciplinary team - our colleagues such physicians, RTs, and RNs about these issues? How can we encourage courageous conversations?
If your hospital doesn't already have a developmental care rounds, then advocate for that. I've been part of rounds that only cover medical issues and how the family is doing is not addressed at all.
Does your hospital have information on some of the cultural factors that could be at play. Is there data that is up on our unit that references mental health or identity and cultural factors? Starting to try and advocate for those things. Or, bring up these issues to your colleagues when you discuss your caseload. If you are discussing a patient status on an ECMO or VAD or track, you might add, "I was talking to that mother yesterday and she sounded like it was a rough day for her." You can start to shift the culture a little bit. In our hospital, if we get a baby who's transferred from the birthing facility, the chart shows the parent's name and the child's gender. When providers document in the chart and they do not mention the child's name. Make the effort to ask, "What is your child's name?". Put it in your notes. Even little things like that set the standard that these details are important.
Citation
Hoffman, M. (2021). Therapeutic strategies for counseling complex patients within a pediatric critical care setting. Continued - Respiratory Therapy, Article 32. Available at www.continued.com/respiratory-therapy
